


When the FDA issued a COVID-19 emergency use authorization (EUA) in 2020, Dr. Jeff SoRelIe was finishing his residency, taking electives, and working in the University of Texas Southwestern (UT) diagnostics lab. Plans changed quickly in the lab since it is a high-complexity lab and was allowed to do PCR testing. The team needed to decide whether to wait for a commercial wave test or bring a test in house.
They had the right resources to do it internally, including a PCR instrument, an automated extractor, and experience with viral CR extraction processing. Dr. SoRelle was a molecular fellow, and his colleague was a microbiology fellow.
Dr. SoRelle recently shared his experience and insights about assay validation and pre- and post-analytical considerations during a pandemic.

Key takeaways:
- Bringing assays in-house can offer several advantages, including faster turnaround times and better control over the supply chain
- Getting samples and controls early is crucial for successful testing
- Using controls that closely mimic the actual target can improve the accuracy of the assay
Which Assay to Validate?
The CDC had three targets, while Charite, Thermo Fisher, Japan, and Hong Kong University targeted different genome parts. Some groups didn’t disclose what they looked at, and others published their assay designs. The UT team did sequencing and dropouts of certain targets and found that some companies copied the same designs. They decided to go with the CDC targets.
Supply chain challenges made it hard to get many supplies, especially those essential for controls. The team also had to consider extraction, the assay to use, and whether they could get the polymerases. Kits were challenging to find, so they had to put them together.
Cartridges for certain tests were rationed. Without availability, they couldn't do the last critical part of the selection process—controls. Primers were readily available, and labs usually have polymerases ready to use, but having the controls to ensure the chemistry works is much more challenging.
The EUA allowed for contrived clinical specimens. Some people may have chosen to use plasma DNA as this is relatively quick and easy. The caution here is that the CDC did that, and it’s why they had a contamination issue.
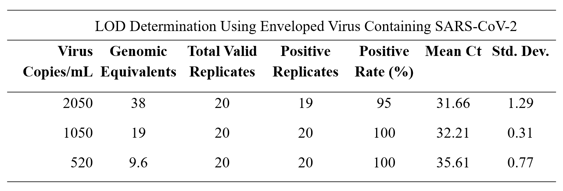
One of the lab’s collaborators, who’d just completed research for the other coronaviruses, was able to get the gene of interest into one of his plasmids and build up RNA. The best thing to work with is encapsulated RNA. There are several options, and each has its pros and cons. The key is an outer protective layer to keep the RNA stable. UT test trialed an AccuPlex product from SeraCare that used an enveloped virus containing SARS-CoV-2. They saw a limited detection curve, detecting 20 different samples for each scenario. With a dilution downwards, they consistently got a positivity rate of 100% at 500 copies per milliliter across all the cases.
Want a more detailed look at the process and performance? Download the webinar recording.
Variant Sequencing & AI

UT performed automated RNA extraction on their coded positive specimens, and they could save mutational signatures unique to each variant. After sequencing, they used an integrated genome viewer browser for informatic analysis. A machine learning program provided the lineage to confirm that their PCR-targeted test was working as well as NGS.
At one point, they had conflicting information about a sample’s mutations. They wondered if the PCR test missed some delta variant mutations, whether it was a hybrid, recombinant, or contamination. Machine learning incorporates artificial intelligence, which introduces the possibility of something being missed or not understood. AI performs based on the data it's been given and trained for. In the end, they could classify it correctly through manual review. It’s vital to update your variance knowledge base almost every week to continue getting correct results.
Dr. SoRelle explained that the UT team learned several lessons, pre-analytic and post-analytic. He shared that it’s a good idea to bring assay in-house to combat the slow external turnaround times, it’s essential to get proper controls, and it's always best to use what is closest to the actual specimen. Ultimately, they got five residual specimens from their Dallas County partners to validate that the test worked. That allowed them to offer it in real-time to their constituents, which included patients, occupational healthcare, and the community.
“Great teams are important,” he said. “We had great people working together and great advice from microbiology and molecular coming together to leverage the instruments and expertise.”
Want a more detailed look at the process and performance? Download the webinar recording.
Ask Dr. SoRelle
Nearly half the webinar was devoted to answering wide-ranging questions from attendees. He covered safety around pooling samples, detecting new variants, testing turnaround times, preparing for the next pandemic, advice for choosing PRC instruments and controls, the quality of antigen testing, and more. To hear the interesting, informative Q&A session, download the webinar.
Jeff SoRelle, M.D., is an assistant professor of pathology and a board-certified molecular genetic pathologist. His clinical research interests include improving quality metrics in genomic medicine and multiplex assays. He completed a molecular genetic pathology fellowship at the University of Texas Southwest Medical Center.